Clinical context
Fasciolosis
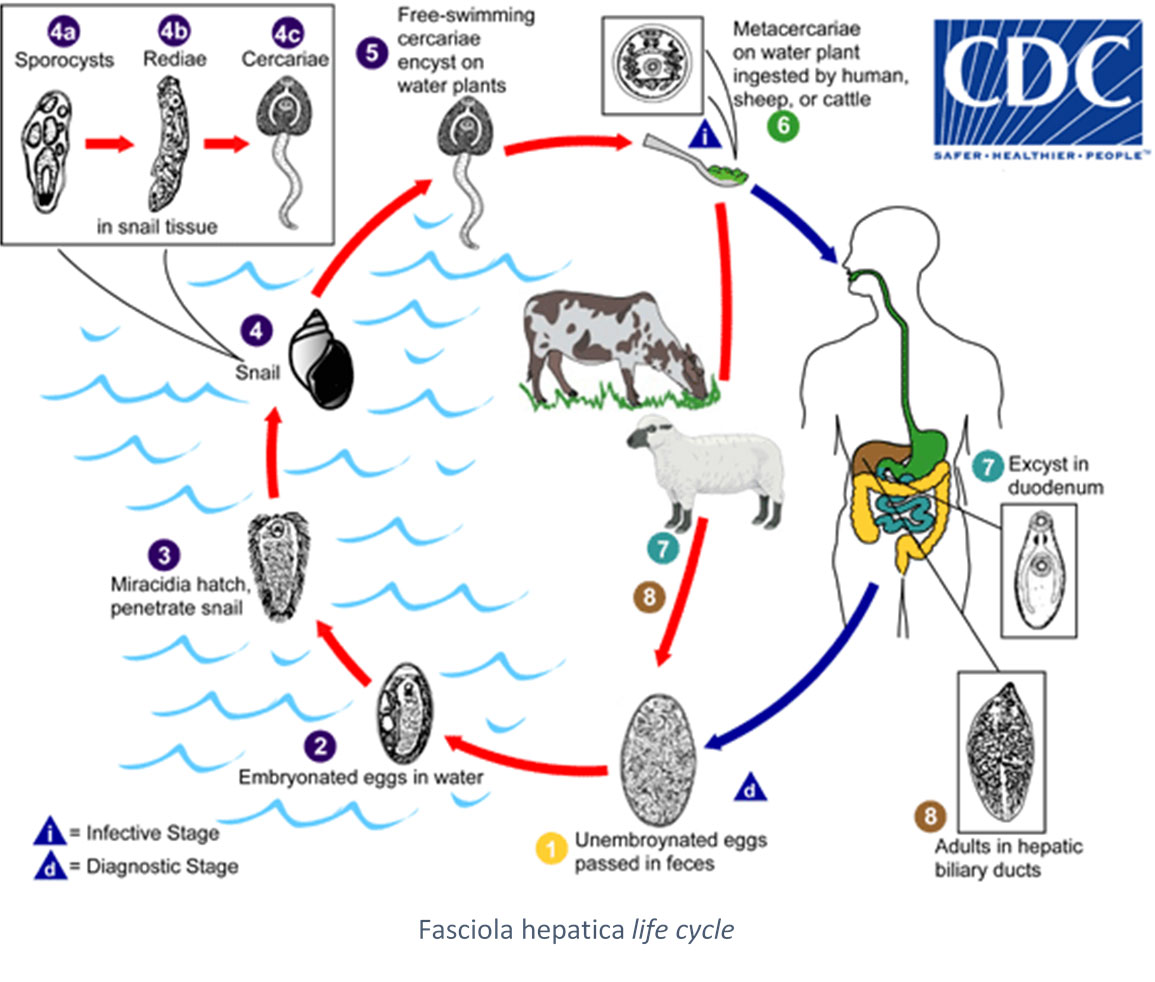 Fasciolosis (hepatic distomatosis) is a zoonosis due to the presence in the organism of trematode worms, commonly known as liver flukes. The species of the Fasciola genus have different life cycles involving different hosts and have a various geographical distribution. Among them, Fasciola hepatica, main agent of fasciolosis is also the most commonly found species, and present worldwide. The adult fluke lives in biliary canals of a wide proportion of mammalians, such as cattle and sheep, while humans are accidental hosts. Adults release a large number of eggs through hosts feces. They hatch in water, releasing a ciliated embryo (myracidium) that penetrates into a snail of the Lymnaea genus. The parasite multiplies into the snail before leaving it as a mobile larva (cercariae) which encysts on water plants (metacercariae). Final host gets infected by ingestion of contaminated plants (water cress, dandelion, chicory…). For the other species of flukes, contamination can occur by ingestion of undercooked fresh water fish or shellfish (Dietrich et al., 2015).
Fasciolosis (hepatic distomatosis) is a zoonosis due to the presence in the organism of trematode worms, commonly known as liver flukes. The species of the Fasciola genus have different life cycles involving different hosts and have a various geographical distribution. Among them, Fasciola hepatica, main agent of fasciolosis is also the most commonly found species, and present worldwide. The adult fluke lives in biliary canals of a wide proportion of mammalians, such as cattle and sheep, while humans are accidental hosts. Adults release a large number of eggs through hosts feces. They hatch in water, releasing a ciliated embryo (myracidium) that penetrates into a snail of the Lymnaea genus. The parasite multiplies into the snail before leaving it as a mobile larva (cercariae) which encysts on water plants (metacercariae). Final host gets infected by ingestion of contaminated plants (water cress, dandelion, chicory…). For the other species of flukes, contamination can occur by ingestion of undercooked fresh water fish or shellfish (Dietrich et al., 2015).
Fasciolosis has two successive clinical stages. The acute invasion phase corresponds to the initial larvae migration to the liver. Patients present fever, abdominal pain, weight loss and hepatosplenomegaly. Myalgia, urticaria and other allergic reactions are also frequent signs. Chronic hepatic phase or state phase, rarely observed in temperate regions, starts 2 to 3 months later, linked to the obstruction of biliary canals by the parasite (bile colic, bacterial secondary infections…) (Harrington et al., 2017).
Other forms of distomatosis can occur with other fluke species, especially pulmonary distomatosis for instance, due to worms of the Parogonimus genus. Ectopic forms have also been described in the case of the infection of another organ by the parasite (Taghipour et al., 2019).
Cosmopolitan parasitosis, fasciolosis has a renewed interest in the north hemisphere, as the epidemiology of this highly pathogenic reemerging infection has evolved these past few years. F. hepatica, the infectious agent found in Europe not the sole species detected anymore due to migratory flux and tourism. According to WHO, 2.4 million people, mostly children, are infected by F. hepatica and millions of other at risk worldwide (WHO). These contaminations are directly linked to local customs and hygiene conditions encountered (Webb et al., 2018). It is also possible that prevalence increases with the rise in temperature (Vignoles et al., 2017). In France, cases remain rare and sporadic.
Diagnosis is done according to epidemiological data, patient history, clinical signs, imaging and biological results (direct examination of eggs, antigenemia, copro-antigen research and serology). Serological techniques can use raw, Excretory/Secretory (ES) or recombinant antigens (Webb et al., 2018).
SCIENTIFIC REFERENCES
- Agnamey P, Fortes-Lopes E, Raccurt CP, Boncy J, Totet A. Cross-sectional serological survey of human fascioliasis in haiti. J Parasitol Res. 2012;2012:751951.
- Arafa MS, Abaza SM, El-Shewy KA, Mohareb EW, El-Moamly AA. Detection of Fasciola-specific excretory/ secretory (E/S) protein fraction band (49.5 kDa) and its utilization in diagnosis of early fascioliasis using different diagnostic techniques. J Egypt Soc Parasitol. 1999;29(3):911–26.
- Hotez PJ, Savioli L, Fenwick A. Neglected tropical diseases of the Middle East and North Africa: review of their prevalence, distribution, and opportunities for control. PLoS Negl Trop Dis. 2012;6(2):e1475.
- Khan MK, Sajid MS, Riaz H, Ahmad NE, He L, Shahzad M, et al. The global burden of fasciolosis in domestic animals with an outlook on the contribution of new approaches for diagnosis and control. Parasitol Res. 2013 Jul;112(7):2421–30.
- Maciel MG, Lima WDS, de Almeida FLM, Coelho LIARC, Araújo GAN, Lima MG, et al. Cross-Sectional Serological Survey of Human Fascioliasis in Canutama Municipality in Western Amazon, Brazil. J Parasitol Res. 2018;2018:6823638.
- Mera y Sierra R, Agramunt VH, Cuervo P, Mas-Coma S. Human fascioliasis in Argentina: retrospective overview, critical analysis and baseline for future research. Parasit Vectors. 2011 Jun 11;4:104.
- Rondelaud D, Dreyfuss G, Bouteille B, Dardé ML. Changes in human fasciolosis in a temperate area: about some observations over a 28-year period in central France. Parasitol Res. 2000 Sep;86(9):753–7.
- Salimi-Bejestani MR, McGarry JW, Felstead S, Ortiz P, Akca A, Williams DJL. Development of an antibody-detection ELISA for Fasciola hepatica and its evaluation against a commercially available test. Research in Veterinary Science. 2005 Apr 1;78(2):177–81.
- Youssef AI, Uga S. Review of Parasitic Zoonoses in Egypt. Trop Med Health. 2014 Mar;42(1):3–14.
FASCIOLA ES Western Blot IgG TEST
The Western Blot technique has been widely used in recent years for the diagnosis of fasciolosis. It allows the diminution of cross-reaction risks compared to other serological techniques (Mezo et al., 2003).
The Haute Autorité de Santé (HAS) in France as well as the American Center for Disease Control (CDC) recommend the immunoblot for the confirmation of serodiagnoses (Argumentaire HAS, 2018, DPDx CDC, Fasciolasis, 2019). Serological follow-up is indicated in case of diagnosis during the acute invasion phase of the disease.
In order to answer the demand, we developed a reliable test based on the Western Blot technique. Associated with highly sensitive natural ES antigens, the FASCIOLA ES Western Blot IgG test is a robust confirmation technique of classical screening tests for the diagnosis of fasciolosis.
Our products
Order
To order a product, please send us an email to our address Order with the description of the product. We ship worldwide.
