Clinical context
Chagas disease
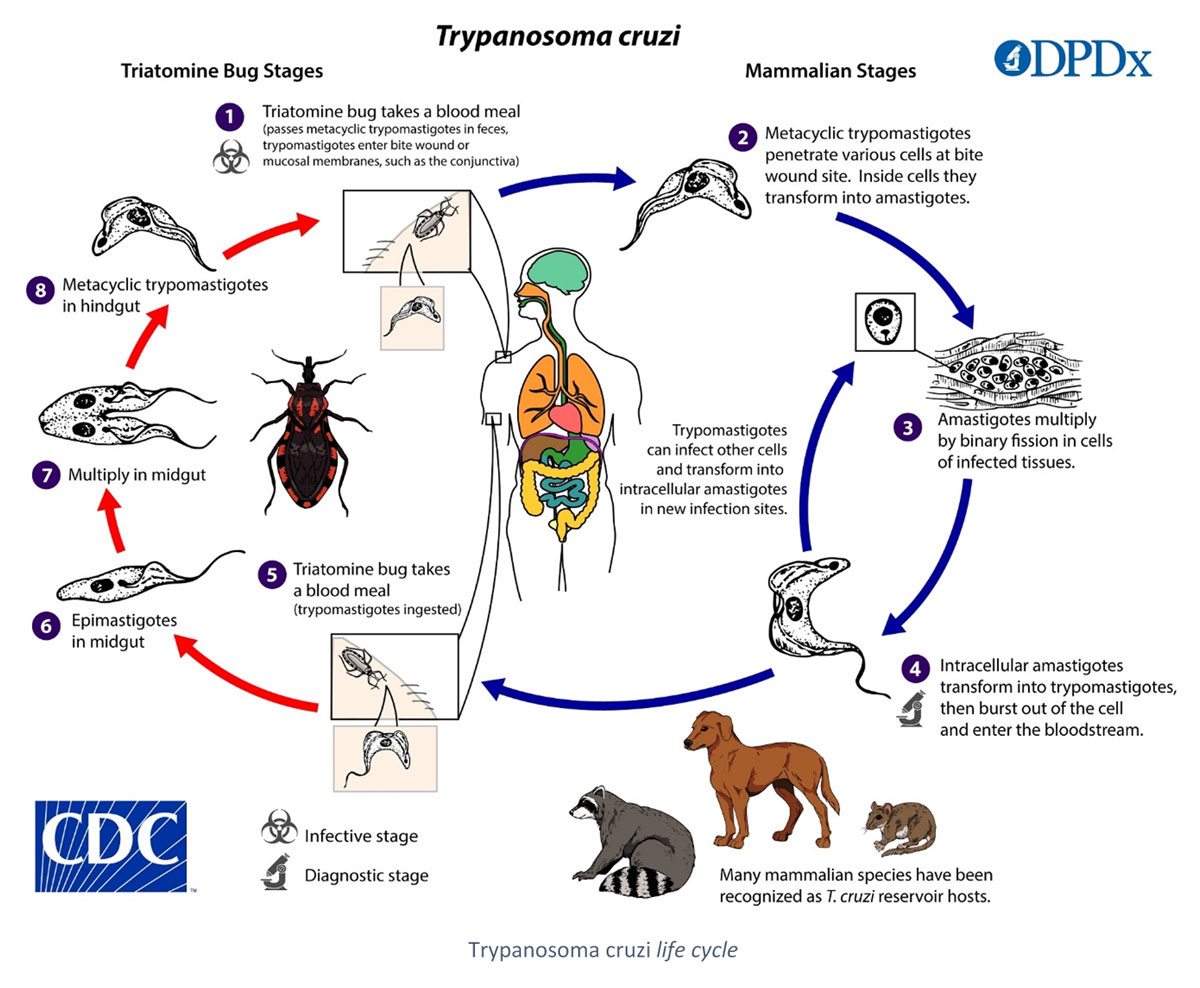 Chagas disease (or American trypanosomiasis) is a parasitosis caused by the protozoan Trypanosoma cruzi, an hematophagous vector, the triatominae (or kissing bug), and humans. Contamination can occur directly after the bite of the insect, more precisely when the patient scratches the lesion, which put the contaminated dejections of the bug in contact with the patient’s blood. Ingestion of contaminated fruits of vegetables can also lead to a contamination. Blood transfusion, organ transplantation and congenital transmissions are possible. This zoonotic infection affects numerous species of both wild and domestic mammalians (cats and dogs included).
Chagas disease (or American trypanosomiasis) is a parasitosis caused by the protozoan Trypanosoma cruzi, an hematophagous vector, the triatominae (or kissing bug), and humans. Contamination can occur directly after the bite of the insect, more precisely when the patient scratches the lesion, which put the contaminated dejections of the bug in contact with the patient’s blood. Ingestion of contaminated fruits of vegetables can also lead to a contamination. Blood transfusion, organ transplantation and congenital transmissions are possible. This zoonotic infection affects numerous species of both wild and domestic mammalians (cats and dogs included).
Life cycle of the parasite is complex, including several stages in the vector as well as in the hosts. Once in the bloodstream of the host, the parasite migrates to different tissues. The triatominae infects itself during the blood meal on a contaminated host. Clinical signs are linked to the parasite itself and the immune response of the host (Rassi et al., 2010).
Chagas disease usually has two clinical phases, acute and chronic. Acute phase corresponds to the spread of the parasite into the different tissues (muscles, liver, intestines, heart…). The patient may have some weak symptoms, but is often asymptomatic. When symptomatic, the first characteristic visible sign is a cutaneous lesion or a purplish edema of the eyelid. Heart or brain acute damages are sometimes observed and can be lethal.
In 60% of cases, a more severe clinically chronic phase occurs, after an undefined asymptomatic period. Depending on the location of the parasite, different organs can be affected. Some patients develop isolated digestive forms, but the cardiac form is the most common one, leading to potentially lethal cardiomyopathies, with a high risk of cerebrovascular accidents. Nervous system forms are also observed, with very poor prognosis (Echeverria & Morillo, 2019).
The WHO estimates that 7 million persons are infected worldwide. Chagas disease is mostly present in Latin America, where it is endemic, but it tends to spread in North America and Europe with the increasing migratory flux and climate changes. It is an importation disease considered and it is classified as a neglected tropical disease (NTD) since 2008 (WHO).
As the acute phase is characterized by a high parasitemia, diagnosis initially relies on its direct observation (microscopy on blood samples) and/or DNA detection (PCR). In the case of congenital American trypanosomiasis, diagnosis is also performed via direct detection techniques, including PCR.
Diagnosis of chronic forms relies on serology. The most commonly used methods are indirect immunofluorescence, hemagglutination and ELISA. However, these tests lack specificity and require confirmation tests (Pérez-Molina & Molina, 2018).
SCIENTIFIC REFERENCES
- Abras A, Gallego M, Llovet T, Tebar S, Herrero M, Berenguer P, Ballart C et al. Serological Diagnosis of Chronic Chagas Disease: Is It Time for a Change? J Clin Microbiol 2016 54, 1566–1572
- Abras A, Muñoz C, Ballart C, Berenguer P, Llovet T Herrero M, Tebar S et al. Towards a New Strategy for Diagnosis of Congenital Trypanosoma cruzi Infection. J Clin Microbiol 2017 55, 1396–1407
- Angheben A, Boix L, Buonfrate D, Gobbi F, Bisoffi Z, Pupella S, Gandini G et al. Chagas disease and transfusion medicine: a perspective from non-endemic countries. Blood Transfus 2015
- Capuani L, Bierrenbach A Pereira Alenca A, Mendrome A Jr, Ferreira JE, Custer B, P Ribeiro AL et al. Mortality among blood donors seropositive and seronegative for Chagas disease (1996–2000) in São Paulo, Brazil: A death certificate linkage study. PLOS Negl Trop Dis 2017 11, e0005542
- De Nova BA, Gonzales ON. An ecological overview on the factors that drives to Trypanosoma cruzi oral transmission. Acta Trop 2015 151, 94–102
- Pinazo M-J, Gascon J. The importance of the multidisciplinary approach to deal with the new epidemiological scenario of Chagas disease (global health). Acta Trop 2015 151, 16–20
- Sales Junior PA, Molia I, Fonseca Murta SM, Sanchez-Montalva A, Salvador F, Corrêa-Oliveira R, Carneiro C. Experimental and Clinical Treatment of Chagas Disease: A Review. Am J Trop Med and Hyg 2017 97, 1289–1303
- Soriano-Arandes A, Angheben A, Serre-Delcor N, Treviño-Maruri B, Gómez I Prat J, Jackson Y. Control and management of congenital Chagas disease in Europe and other non-endemic countries: current policies and practices. Trop Med Int Health 2016 21, 590–596
CHAGAS WESTERN BLOT IgG TEST
The WHO and the American CDC recommend the use of two serological techniques for the diagnosis of chronic forms of Chagas disease, including immunoblot (DPDx American trypanosomiasis, 2019).
In order to answer the demand, we developed a reliable test based on the Western blot technique. Associated with highly sensitive natural antigens, the CHAGAS Western blot IgG test is a robust confirmation technique of classical screening tests.
The excellent performances of the Western blot technique would allow the diagnosis of congenital Chagas disease in children several months after birth (Abras et al., 2017).
Its high specificity also ensure a low risk of cross-reaction, including regarding species of the Leishmania genus (Pérez-Molina & Molina, 2018, Abras et al., 2016).
Our products
Order
To order a product, please send us an email to our address Order with the description of the product. We ship worldwide.
