Clinical context
Cysticercosis
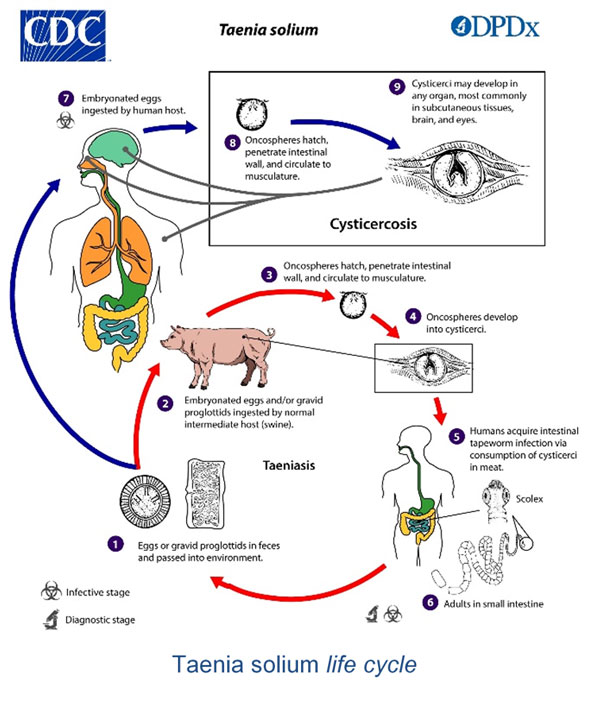 Cysticercosis is a helminthiasis due to the development of Taenia solium larval cysts. Human is the only definitive host of this cestode, with the adult worm developing in the intestine and spreading eggs into the environment. These eggs are directly infectious for intermediate hosts, usually pigs, but also for humans who then become a parasitical deadlock. Human is usually infected by ingestion of water or vegetables contaminated by eggs. Contamination can sometimes result from an auto-infestation, either by the fecal-oral route or by digestion of proglottids that moved back into the gastric area either due to their own mobility or intestinal anti-peristalsis (Gonzales et al., 2016).
Cysticercosis is a helminthiasis due to the development of Taenia solium larval cysts. Human is the only definitive host of this cestode, with the adult worm developing in the intestine and spreading eggs into the environment. These eggs are directly infectious for intermediate hosts, usually pigs, but also for humans who then become a parasitical deadlock. Human is usually infected by ingestion of water or vegetables contaminated by eggs. Contamination can sometimes result from an auto-infestation, either by the fecal-oral route or by digestion of proglottids that moved back into the gastric area either due to their own mobility or intestinal anti-peristalsis (Gonzales et al., 2016).
Once ingested, eggs release embryos which cross the intestinal mucosa and reach the circulatory system before migrating in several anatomical areas. Larvae mainly infect subcutaneous tissue, muscles, eyes and Central Nervous System. Muscular and subcutaneous cysticercoses are usually clinically quiet and discovered accidentally, but cerebral and ocular forms are more severe and require a medical and rarely surgical support, before the calcification of the lesions. The sooner the treatment begins, the less will be risk of sequelae. Young larvae, which do not trigger an inflammatory reaction, are not detected by CT scan. They can degenerate in a couple weeks or more slowly, releasing antigens and generating a peripheric granulomatous reaction (ring aspect on cerebral CT scan) (Garcia et al., 2003).
Ocular cysticercosis is clinically revealed by inflammatory reactions or tumoral signs that vary according to the anatomic location of the larva. Neurocysticercosis can be suspected with epilepsy (parenchymatous neurocysticercoses), intracranial hypertension (subarachnoid cysticercoses and brain racemous forms) or hydrocephalus (ventricular cysticercoses). Neurocysticeroses may be responsible of 3 to 8 million of epilepsy cases worldwide (WHO, 2015).
Considered as a neglected tropical disease (NTD), cysticercosis remains a major public health issue. The disease is widely spread in developing countries, especially in tropical and subtropical areas, where it concerns more than 50 million people. Prevalence is the highest in Latin America (5-10%), but cysticercosis is also very present in central and south Africa, around the Indian Ocean, in southern-east Asia and in China. In these areas, the infection is linked to the presence of traditional pig farming without veterinary control and with poor hygiene (Braae et al., 2018).
Cysticercosis is currently becoming a growing issue in developed countries, especially in Europe and North America, where reported cases are increasing because of globalization and migration of asymptomatic carriers of adult Taenia worms from endemic areas (Zammarchi et al., 2013, Symeonidou et al., 2018).
Because of non-specific clinical manifestations and very long interval for the appearance of symptoms after contamination, diagnosis is difficult. Direct parasitological diagnosis is rarely possible as biopsies are invasive. With indicative epidemiological context and clinical signs, morphological exams (scan, MRI), although expensive and not always accessible in endemic areas (Gomez-Morales et al., 2017), are crucial for the diagnosis. The diagnostic must be immunologically confirmed by serology on serum or cerebrospinal fluid.
SCIENTIFIC REFERENCES
- Deckers N, Dorny P. Immunodiagnosis of Taenia solium taeniosis/cysticercosis. Trends Parasitol. 2010 Mar;26(3):137–44.
- Del Brutto OH. Diagnostic criteria for neurocysticercosis, revisited. Pathog Glob Health. 2012 Sep;106(5):299–304.
- Dournon N, Epelboin L, Brion M-C, Paris L, Bricaire F, Caumes E. Seroconversion of neurocysticercosis occurring after anti-helminthic treatment. J Travel Med. 2012 Dec;19(6):383–6.
- Garcia HH, Nash TE, Del Brutto OH. Clinical symptoms, diagnosis, and treatment of neurocysticercosis. Lancet Neurol. 2014 Dec;13(12):1202–15
- Gekeler F, Eichenlaub S, Mendoza EG, Sotelo J, Hoelscher M, Löscher T. Sensitivity and specificity of ELISA and immunoblot for diagnosing neurocysticercosis.n Eur J Clin Microbiol Infect Dis 2002 21(3):227-229.
- Michelet L, Fleury A, Sciutto E, Kendjo E, Fragoso G, Paris L, Bouteille B. Human neurocysticercosis: comparison of different diagnostic tests using cerebrospinal fluid. J Clin Microbiol 2011 49(1):195–200.
- Mwang’onde BJ, Nkwengulila G, Chacha M. The Serological Survey for Human Cysticercosis Prevalence in Mbulu District, Tanzania. Adv Infect Dis 2012 02(03):62–66.
- Raccurt CP, Agnamey P, Boncy J, Henrys JH, Totet A. Seroprevalence of human Taenia solium cysticercosis in Haiti. Raccurt CP, Agnamey P, Boncy J, Henrys JH, & Totet A, J Helminthol 2009 83(2):113–116.
- Rodriguez S, Wilkins P, Dorny P. Immunological and molecular diagnosis of cysticercosis. Pathog Glob Health. 2012 Sep;106(5):286–98.
- Salazar-Anton F, Tellez A, Lindh J. Evaluation of an immunodot blot technique for the detection of antibodies against Taenia solium larval antigens. Parasitol Res 2012 110(6):2187–2191.
- Šoba B, Beović B, Lužnik Z, Skvarč M, Logar J. Evidence of human neurocysticercosis in Slovenia. Parasitology 2014 Apr;141(4):547-53.
- van Doorn HR, Wentink-Bonnema E, Rentenaar RJ, van Gool T. Specific cross-reactivity in sera from cystic echinococcosis patients in an enzyme-linked immunoelectrotransfer blot for cysticercosis diagnostics. Trans R Soc Trop Med Hyg. 2007 Sep;101(9):948–50.
CYSTICERCOSIS Western Blot IgG TEST
Even though ELISA is the most commonly used screening test, it lacks sensitivity, in particular for parenchymatous neurocysticercoses. Moreover, there is a high risk of cross-reactions with other parasites, especially in developing countries where polyparasitism is common.
The Haute Autorité de Santé (HAS) in France as well as the American Center for Disease Control (CDC) recommend the immunoblot for the confirmation of serodiagnoses (Argumentaire HAS, 2018, DPDx Cysticercosis, 2019).
Immunoblot is the serological test with the best performances in terms of sensitivity and specificity (Rodriguez et al., 2012, Deckers et al., 2010). It allows an early diagnosis, when patients are more susceptible to be receptive to treatment.
In order to answer the demand, we developed a reliable test based on the Western Blot technique. Associated with highly sensitive natural antigens, the CYSTICERCOSIS Western Blot IgG test is a robust confirmation technique of classical screening tests for the diagnosis of cysticercosis and neurocysticercosis.
Performance evaluations of CYSTICERCOSIS Western Blot IgG test on several sample cohorts showed a 97,5% sensitivity and a specificity of 100% including with patients suffering of different parasitoses or auto-immune diseases.
Our products
Order
To order a product, please send us an email to our address Order with the description of the product. We ship worldwide.
